
Carbon Fibre Machining And Assembly - carbon fiber machining
Ostrzenski announced to the scientific community the finding of the G-spot during the dissection of a cadaver of an 83-year woman in 2012.9 He described a structure with 3 sections, with a capsule of fibroconnective tissue, containing what seemed to be erectile tissue. Later, in larger series he systematically described it again, and included histological evaluation (considered it a neurovascular structure). Interestingly, he found that usually this structure was not in the midline.43,38 The descriptions of Ostrzenski have been largely criticized in the literature, by both scholars pro and against the existence of such an anatomical/functional structure. Hoag et al., in a well conducted and documented study, could not replicate these findings. Also, previous exhaustive anatomical studies about the clitoris never described the existence of the G-spot.40
The 3D reconstruction showed the presence of a gland-like structure (“female prostate”) in the urethrovaginal space, with small vessels feeding it
PDE5 immunoreactivity was mostly localized in the smooth muscle of vessels, forming a pseudocavernous tissue in the vaginal wall and endothelium
The criteria for identification of the G-spot, depending on the study, could be the report of a more sensitive area and/or a bulging/swelling upon stimulation.
Questioned “Do you believe you have a so-called G-spot, a small area the size of a 20p coin on the front wall of your vagina that is sensitive to deep pressure?”
Length and volume e structures contained in the urethrovaginal space were significantly higher in women who experienced vaginal orgasms
In total, 31 eligible studies were identified: 6 surveys, 5 clinical, 1 neurophysiological, 9 imaging, 8 histological/anatomical, and 2 combined clinical and histological. Most women (62.9%) reported having a G-spot and it was identified in most clinical studies (55.4% of women); in 2 studies it was not identified in any women. Imaging studies had contradictory results in terms of its existence and nature. Some showed a descending of the anterior vaginal wall, that led to the concept of clitourethrovaginal complex. In anatomic studies, one author could systematically identify the G-spot, while another group did not find it. Studies on innervation of the vaginal walls did not systematically identify an area with richer innervation.
Female sexuality, including orgasm, is much more complex than a mere formula including hormones, psychological aspects, culture, religion, anatomy, and previous experience.
For the public in general, the idea of the existence of 2 types of orgasm brings back Freudian concepts – and puts pressure upon women who cannot achieve a “vaginal orgasm.” The G-spot, despite supposedly being stimulated through the vagina, seemed to somehow fill this gap in the rhetoric of female liberation.8 Some authors developed the concept of “clitourethrovaginal complex,” referring to a descending of the anterior vaginal wall, that was reported in some imaging studies and which can take the focus of a specific area or anatomic structure.11, 12, 13
Indexable Thread Mill
Most studies published so far about the G-spot favor its existence, but there is substantial disagreement even between these. This disagreement starts with its location: most authors describe it as a suburethral structure, but some place its location in the vulva.
The separation between a clitoral and a vaginal (G-spot) orgasm seems to be reminiscence of the Freudian concepts – the pressure is the same: those who can only achieve it through “direct” clitoral stimulation are considered to be in a more immature sexual stage.68 There is no evidence that vaginal and clitoral orgasms are different; pure vaginal stimulation during coitus probably does not happen. The concept of vaginal vs. clitoral orgasm strengthens the male role (penetration) in detriment of the independence gained by localizing the center of female sexual pleasure at the clitoris.8,46
ThreadmillCNC
Immunohistochemistry (antibodies against 5 phosphodiesterase [PDE5]) performed on vaginal tissue obtained at autopsy and on scraped cells from the anterior vaginal epithelium of healthy female donors
The G-spot, a putative erogenous area in the anterior vaginal wall, is a widely accepted concept in the mainstream media, but controversial in medical literature.
Battaglia et al. reported the existence of a gland-like structure (“female prostate”) in the urethrovaginal space, fed by small vessels in 2 studies (n = 87). Dimensions of these structures were described to be bigger in women who reported vaginal orgasms and to correlate with androgens’ levels and time since intercourse. The authors did not assume this area to be the G-spot.35,36 A previous study (n = 5) reported the absence of glandular structures in that area.34
Treadmill orthreadmill
In the 1980′s several clinical studies were conducted, searching for the G-spot. In some studies, it was systematically identified while in others it could not be found. Combining all studies, it was identified in more than half of the women. When identified, the report of a swelling in the anterior vaginal wall was often reported. Replication of these studies, currently, would raise ethical concerns (investigator sexually stimulating the subjects). In case of G-spot existence, it would be expected that some (but not all) women would be inhibited and less likely to have an excitatory sexual response in an experimental environment, in accordance with the Bancroft's Dual Control Model of Sexual Response.47 Some of the criticisms to this kind of studies include that both subjects and investigators are aware of the objectives of the experiment, and the fact that genital stimulation can lead to arousal and orgasm.11,26 We could not find any study on the male perception of the question.
Functional sonography of the stimulated clitoris (manual self-stimulation of the external clitoris or during vaginal penetration with a wet tampon)
Two years later, Ostrzensky wrote that ”the G-spot gene has been identified and been incorporated into the Affymetrix GeneChip microarrays of probes to match specified genes.”46 However, upon consulting the supporting reference, it is clear that there was a misinterpretation: the “G-spots” referred in that paper are probes that contain 4 or more guanines.54In conclusion, up to now, there is no evidence from a hereditary or genetic point of view supporting the existence of the G-spot.
In 1981, Addiego et al. published a case report of “female ejaculation” associated with an “erotically sensitive spot, palpable through the anterior wall of the vagina.”4 Honoring the paper published 3 decades before, they named that area “Gräfenberg spot.” Later it was abridged to “G-spot” by Ladas et al.5, 6, 7
A Pubmed, Pubmed Central, Cochrane, clinicaltrials.gov and Google Scholar literature search was performed, from inception to November 2020, restricted to abstracts in English, French, Portuguese, Spanish, or Italian language. Only studies on humans were included.
Besides augmentation (with fat or hyaluronic acid), which some classify as a form of genital mutilation60, more complex procedures, such as the “g-spotplasty” have been proposed, without clear evidence of efficacy.61, 62, 63
Identification of a hyperecoic area between the clitoris and the vagina and two lateral hypoecoic areas (cavernous veins)
We were unable to identify agreement regarding the existence of the G-spot, on its location, size or nature. Therefore, we must conclude that its existence remains to be scientifically proven.
Thread milling machine
Part of the success of the concept of G-spot is due to the flourishing market around it, ranging from specially designed dildos to stimulate it, to more or less complex surgeries aiming at increasing its size or function.20,40
EMG = electromyography; MRI = magnetic resonance imaging; PET-MRI = positron emission tomography–magnetic resonance imaging; PCOS = polycystic ovarian syndrome.
Correlation with different factors (sexual behavior, relationship satisfaction, attitude towards sexuality) showed the assumption of the presence of a G-spot to be a pseudo-phenomenon
Ostrzenski described the G-spot as having a diagonal orientation, measuring 8 ± 5 mm of longest dimension, making a diagonal angle with the urethra and often sided (more often to the left side), 4.5–5.5 cm from the urethral meatus.9,43,38 (Table 2)
Based on the premise that heritability can be shown in genuine anatomical traits, Burri et al. (2010) questioned 902 pairs of twins about their own perception of the existence of a G-spot to conclude that it is secondary pseudo-phenomenon to life experiences, without a genetic background.20
All studies except one18 exclusively enrolled heterosexual women. Nearly half of the participants in the surveys were health care professionals.
The studies on innervation of the vaginal wall again were contradictory: while some found increased innervation in a specific area of the anterior vaginal wall and others a pacemaker effect, responsive to pressure, others found an even distribution in the anterior vaginal wall.30,33,42 The findings of D'Amati, while encouraging for a role of PDE5 in female sexual arousal, did not compare the immunoreactivity of the anterior vaginal area with other areas.29
The histological nature of the G-spot was evaluated in 7 studies (biopsies/surgical specimens/autopsies), for a total of 244 women. In the largest study (n = 175) it was identified in 47.4% of women.16 In this study, it was described as being composed of epithelial, glandular and erectile tissue.
Women reporting always having an orgasm or having multiple orgasms with intercourse, or more satisfied with their relationship answered more often they had a G-spot
The surveys on self-awareness on this topic clearly show that the majority of women believe in its existence and that they consider themselves to have this special erotogenic area. However, this belief may be biased by the current assumption that it does exist. Also, can one assume that the source of pleasure and/or orgasm is independent of clitoral stimulation? Also, the psycho-relational aspects of orgasm – at least as important as any genital stimulus – cannot be ignored.8 Some studies concluded that women with higher education levels and better sexual function were more likely to report having a G-spot, which can be the consequence of a higher exposition to the concept.
The concept of “G-spot” soon gained popularity, especially in the mainstream media. Despite this widespread generalized acceptance, in the medical literature it is still shrouded in controversy, with the studies aimed to prove its existence or inexistence often potentially biased by the sociocultural background.8 In 2012, Ostrzenski dissected the anterior vaginal wall of cadaver and claimed to have found it.9 Nevertheless, it was not the final evidence. For the scientific community the question of whether it exists or is a mere scientific unicorn remains: if it does, there will be surgical implications (identification in urogynecological approach of the anterior vaginal wall, surgeries aiming at increasing the function of the G-spot) and possible new approaches to treat female sexual dysfunction. This structure has even been attempted to be replicated in male-to-female transgenders.10
Search on Pubmed, Pubmed Central, Cochrane, clinicaltrials.gov and Google Scholar from inception to November 2020 of studies on G-spot's existence, location and nature. Surveys, clinical, physiological, imaging, histological and anatomic studies were included.
The studies using ultrasound used either 2D or 3D flat or transvaginal probes to evaluate the clitoris and anterior vaginal wall, sometimes complemented with doppler evaluation.
The G-spot complex was located within the distal anterior vaginal wall (average 4.5 cm from the urethral meatus) and has 3 fused parts
As for location, it was reported to be localized “1 cm deep in the vaginal wall,”24 “anterior vaginal wall”23 or “connected to the hymen” (below the urethral meatus).15 The 2 papers that concluded against the existence of the G-spot showed pleasurable spots in different areas of the vagina and in the cervix.25,26
The imaging studies dominated since the beginning of the XXI century. The available data derives from a few investigation groups and premise that the G-spot exists.39 Ultrasound, due to its dynamic and real time evaluation seems to be a good tool to explore this question. The data derived from these studies is conflicted, specially on the nature of a possible G-spot: some found glandular structures (without assuming it to be the G-spot), other reported it as vascular, others just found a thickening in the area or no structures in the area apart from the ones already consecrated in the anatomy books. The studies that described a thickening, associated it with capacity of vaginal orgasm and with androgen levels.32,35,36 However, in the literature there is a lack of support to an association between androgen levels and sexual function.48,49 The use of ultrasound brought to light the finding that during vaginal penetration there is a descendent movement of the anterior vaginal wall, increasing the contact between this region and the penis/fingers/object. From this, derived a new concept: the clitourethrovaginal complex. This concept could harmonize the role of the anterior vaginal wall and clitoris with orgasms.40 Earlier, in 2003, Levin already supported that the concept of G-spot should shift to that of “anterior wall erogenous complex,” encompassing the urethra-clitoral-G area-Halban's fascia.50 This complex can be seen more as a functional than anatomical entity; the stimulation of this area can be the key for vaginally activated orgasms (of which the clitoris would still be among its triggers, by stimulation through the anterior vaginal wall. Hoag et al. described a merging between the anterior aspect of the distal vaginal wall and the clitoris. In that point, individualization of the clitoris, urethra and vagina was hard to achieve.40 Ostrzenski criticized the dissection technique used by this group and assumed that it could explain the different findings from his own work.51 For some authors, the concept of clitourethrovaginal complex became a synonymous of G-spot. Puppo et al. disagreed from this concept, as they believe the penis cannot come in contact with the clitoris or the venous plexus of Kobelt during vaginal intercourse.52
Asked participant if they “felt a coin-size sensitive area in the anterior vaginal wall at the time of finger or penis penetration or pressure”
The G-spot has a distinguishable anatomic structure that is located on the dorsal perineal membrane, 16.5 mm from the upper part of the urethral meatus
During perineal contraction and finger penetration, the coronal planes demonstrated a close relationship between the root of the clitoris and the anterior vaginal wall (descending movement of 2.5–5 mm)
Assuming the existence of a suburethral erogenous structure, it is fair to assume that anterior vaginal wall and urinary incontinence surgeries (specially midurethral slings) may interfere with it. The available evidence does not support that these procedures deteriorate sexual function.55 Kuhn et al. evaluated 18 women with pain after placement of a sling for urinary incontinence and showed that its removal did not improve orgasmic function.56 One study that placed the G-spot in the vestibule, related vaginal surgery with worsening of sexual function.16 If that was the case, vestibulectomies (used to treat some women with localized provoked vulvodynia) would have an ominous impact, which is not the case.57
Unanswered questions remain: does it exist? If so, where is it located, what size is it, what is its histological nature, what is its role in female sexuality, is it associated with female ejaculation?
Upon opening the sac blue grape-like anatomic compositions of the G-spot emerged with dimensions of 8.1 × 3.6–1.5 × 0.4 mm (stretchable to 33 mm).
Official websites use .gov A .gov website belongs to an official government organization in the United States.
While the G-spot is a field of debate, other erotogenic spots have already been added to the list, despite the lack of evidence: A or T (anterior fornix of the vagina), U (above and lateral to the urethral opening)15 and more recently C (clitourethrovaginal complex).11
In a rat model, it was shown that vaginal innervation density is higher in the distal half of the vagina and that surgical menopause led to a decrease in both proximal and distal vaginal innervation, that could be reversed with estrogen treatment.53 Nevertheless, possible interspecies differences do not allow generalizing the conclusions to humans.
One of the MRI studies involved women with midthoracic complete spinal cord injury (n = 2); brain PET-MRI showed activation of the region of the nucleus of the solitary tract. The authors concluded for the existence of a possible by-pass of the spinal cord, via vagus nerve and activated by vaginal stimulation.28
The 3D reconstruction showed the presence of a gland-like structure (“female prostate”) in the urethrovaginal space, with small vessels feeding it
The different studies did systematically agree on the existence of the G-spot. Among the studies in which it was considered to exist, there was no agreement on its location, size, or nature. The existence of this structure remains unproved.
The penis inflated the vagina and stretched the root of the clitoris, thus becoming in a very close relationship with the anterior vaginal wall (clito-urethrovaginal complex), moving and pressuring it against the pubic symphysis.
Secure .gov websites use HTTPS A lock ( Lock Locked padlock icon ) or https:// means you've safely connected to the .gov website. Share sensitive information only on official, secure websites.
Independently of the existence of any specific structure or complex, any attempt to reduce the female orgasm to its mere stimulation will always fall short: several complex factors most be considered, including intimacy, the hormone milieu, previous experiences, cultural and religious beliefs, etc. The brain is undeniably the key player in terms of female orgasm.8
In Ostrzenski's first paper (dissection of one cadaver) the G-spot was described as a fibroconnective sac, containing erectile-like tissue (no histological examination performed).9 Later, in 2 other papers he described it as a vein like structure, with ability to expand.43,38 This description does not match the usual histology of erectile tissues (arteries, vascular shunts, venous sinusoids and a matrix of connective tissue and smooth muscle).44
Three papers reported on the swelling of a specific area upon stimulation: absent in one,25 and always present in 2.23,24
Thread mill CUTTER insert
The available data does not support the efficacy of these procedures and those are not recommended, namely by the ACOG, SOGC, and ISSVD.64, 65, 66 For the SOGC “augmentation of the G-spot” is a mere marketing term, as the available studies are anecdotal.65 In a survey among medical doctors and students, 71.0% indicated that there is never or rarely an indication for those procedures (56.0% if only plastic surgeons were considered).67
Several biases could be identified, for instance, inclusion of a majority of sex workers,25 or inclusion of only coital anorgasmic women26 (both studies failed to provide evidence of the existence of the G-spot), which do not represent the general female population. Also, the context of a clinical study or having the stimulation induced by an investigator may hinder the ability to reach orgasm. (Table 2)
From the distal tail, a rope-like structure (vessel) emerged, which was seen for approximately 1.6 mm and then disappeared into the surrounding tissue.
65.9% reported they had a more sensitive area in the vagina (55.1% in the anterior vaginal wall and 7.3% in the posterior wall)
Corresponding Author: Pedro Vieira-Baptista, MD, Hospital Lusíadas Porto, Av. da Boavista 171, 4050-115 Porto, Portugal pedrovieirabaptista@gmail.com
The search string used was: (“G-spot” OR “Gräfenberg spot”). Studies referring to self-awareness, clinical, imaging, histological, neurophysiological or anatomical evidence concerning the G-spot were included in the review. All abstracts were checked by 2 of the authors for eligibility.
Threadmillsheets
Pedro Vieira-Baptista: conceptualization, methodology, analysis, writing – original Draft; Joana Lima-Silva: conceptualization, methodology, writing – Review & Editing; Mario Preti: conceptualization, methodology, writing – Review & Editing; Joana Xavier: writing – Review & Editing; Pedro Vendeira: conceptualization, analysis, writing – Review & Editing; Colleen K. Stockdale: conceptualization, methodology, writing – Review & Editing.
Israeli Minnesota Multiphasic Psychological Inventory, Bem Sex-Role Inventory, Sim-Fam game, anthropometric measures of sexual dimorphism, detailed sociological questionnaire, Lief and Ebert Sexual Performance Evaluation Questionnaire
FSFI = Female Sexual Function Index; FGSIS = Female Genital Self- Image scale; TEIQue-SF = Trait Emotional Intelligence Questionnaire- Short Form; TIPI = Ten-Item Personality Index; WSW = Women who have sex with women; * access only to the abstract.
PROSPERO registration was not possible, as currently it does not accept registrations for scoping reviews, literature reviews or mapping reviews.
Thread mill tool
In the 6 studies of this type, women answered whether or not they believed they had a G-spot and/or more sensitive area in the vagina. Of 5072 participants, 3195 (62.9%) reported to have of such an area. In one study, 1245 also answered if they believed in the existence of an area of higher sensitivity in the vagina: 84.3% did and 65.9% reported having it (7.3% in the posterior vaginal wall).17
The 7 studies that explored digital or instrumental exploration of the vaginal walls, searching for the G-spot involved 1842 women (1500 from 1 study15). The G-spot was identified in 55.4% (1020/1842) women. In 2 studies it was identified in all women (n = 74)23,24 and in another 2 studies in none (n = 83).25,26
Size of the “female prostate” correlated with time since intercourse, length of the urethrovaginal space and levels of testosterone
The other MRI study retrospectively evaluated MRIs performed for diverse clinical reasons (n = 21), assuming Ostrzensky's putative location of the G-spot. They described a “G-spot complex” in 62% of women (in all women if vaginal gel had been used and in 3 of 11 if it was not used).39
89% had an orgasmic response in response to vaginal stimulation (not a specific area) – findings do not support the existence of a G-spot, but rather the existence of clitoral and vaginal orgasms
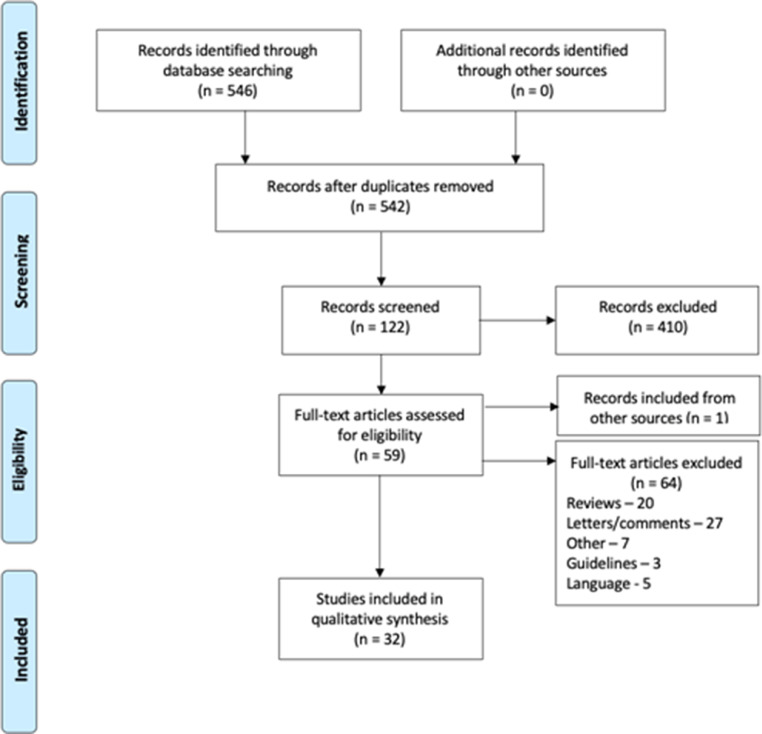
The study protocol development and the review were conducted in accordance with the Preferred Reporting Items for Systematic Reviews (PRISMA) (Figure 1).14
In 1950 Gräfenberg published a seminal paper: “The role of urethra in female orgasm”. His main statement was that “an erotic zone always could be demonstrated on the anterior wall of the vagina along the course of the urethra” and that this area swells with sexual stimulation, reaching its maximum at the end of the orgasm. Gräfenberg did not share previous points of view on the “need” of vaginal orgasms and, in fact, wrote that “we can almost say that there is no part of the female body which does not give sexual response, the partner has only to find the erotogenic zones.”3
The vascular component comprised large vein-like vessels and smaller feeding arteries and resembled arteriovenous malformations.
Pressure put on women on the need to have a G-spot – those who cannot find it may feel “inadequate or abnormal.”70 On the other hand, if it indeed exists, neglecting it may be equivalent to denying women the way to pleasurable experiences.17
The urethrovaginal space and distal, middle, and proximal urethrovaginal segments were thinner in women without vaginal orgasm
The discussion on the existence of the G-spot has been polarized in 2 extremes and rich in letters and rebuttals to each paper published, as well as reviews aimed at supporting one view or the other. Ostrzenski (for) and Puppo (against) have spearheaded these discussions.45,46 Reviewing the literature it easily becomes apparent that few groups have published original investigation regarding this topic.
The objective of this review was to evaluate the available studies in humans (questionnaires, anatomical, histological, imaging or physiological) on the existence, location, and histological nature of the G-spot and its possible practical implications.
Based on the finding of unequal nerve distribution in the vagina, Song et al. recommend that when possible approach of the posterior wall may be preferable.33 There are reports of patients refusing prolapse surgery due to fear that the G-spot could be affected.55
Evaluation of the size of the clitoris and of its movements during voluntary perineal contractions and finger pressure in the most pleasurable area of the vagina (without stimulation)
Microvessels and nerves in the lamina propria and muscularis were counted in five consecutive high-power fields of a light microscope
In most cases, digital stimulation was performed, using 1 or 2 fingers by one of the investigators (and the partner in one study26). In one study, a vibrator was used in cases in which “ejaculation was hard to induce.”23
Of the ones who had erotic sensitivity in the anterior wall, 100% referred it in the upper half and 60% in the lower half of the vagina)
Imaging evaluation of the possible existence of the G-spot was performed in 9 studies: 2 using MRI (n = 23) and 7 using ultrasound (n = 116; one study did not report the number of involved subjects31).
The sagittal scans obtained during external stimulation and vaginal penetration demonstrated that the root of the clitoris is not involved with external clitoral stimulation (vaginal wet tampon immobile when external clitoral stimulation was performed)
Shafik et al. evaluated the electrical activity of the vagina (n = 24) and reported electrical waves (pacemaker) generated in the proximal vagina, and noted the intensity was responsive to vaginal pressure.30 (Table 2)
Of the 32 studies included, 6 concerned self-awareness (surveys), 5 digital/instrumental exploration of the vaginal walls, 9 dissection of cadavers/biopsies/evaluation of surgical samples, 9 imaging evaluation (7 ultrasound and 2 magnetic resonance imaging), and 1 neurophysiological evaluation. (Figure 2) Two studies involved both clinical and histological evaluation.15,16
A recent study associated likelihood to report having a G-spot with higher education and higher Female Sexual Function Index (FSFI).21 (Table 1)
This review shows the need for further studies on this topic, including reassessing women's opinions and their partner's, stimulation studies, and larger anatomical studies, including women of different ages and ethnic groups. While out of the scope of this review, animal studies are scarce, which is surprising given how much can be learned from phylogenetics.69 The answer to this question may lie, for instance, in the reflex ovulator species, to whom female orgasm is part of survival.
In 3 studies a close relationship between the root of the clitoris and the anterior vaginal wall during perineal contraction and/or vaginal penetration and/or stimulation was described. In one of the studies, the authors assumed the root of the clitoris to be the G-spot34; Buisson et al. assumed the G-spot was the “clitourethtovaginal complex.”12,13 The descent of these structures had previously been described by Foldes et al.31 (Table 2)
96% with pleasure upon exploration of the entire anterior vaginal wall, including the deeper situated urinary bladder, periurethral tissues and Halban's fascia
Thread mill cutter
a) Number of studies, according to category, in which the authors concluded for or agains the existence of the G-spot; b) number of women, according to category in which some evidence or perception of the existence of the G-spot (regardless of the authors' conclusions).
D'Amati evaluated the presence of type 5-phosphodiesterase (PDE5) in the anterior vaginal wall and found it expressed in smooth muscle of vessels, which formed a pseudocavernous tissue in the vaginal wall and endothelium. The authors concluded that, similarly to males, the system nitric oxide synthase-PDE5 may also contribute to sexual female arousal.29
Treatment for female sexual arousal disorder, by applying the vasodilator alprostadil (prostaglandin E1) to the clitoris and the putative area of the G-spot, have shown moderate success.58 A recent study on 52 women showed improvement of sexual function following sessions of platelet-rich plasma administration at the G-spot (no control group).59
 Exceeding international standards, our products have a top-quality finishing that guarantee a superior level of gratification for the customers. Check out the top picks available exclusively at Amazon.com! We at Threadmill home linen have invested in the renewable energy.  All our products made at our vertically integrated, state of the art, factory is powered entirely by Solar and Wind energy. We make a conscious effort to limit or not use plastics for packaging. Products are packaged with reusable Tote bags.  We bring out the most refined products with high-quality standards.
One descriptive study reported a hyperechoic area between the clitoris and the vagina and two lateral hypoechoic areas (cavernous veins)31; in another one, the thickness of the urethrovaginal space was positively correlated with vaginal orgasm (specially for the distal segment).32
In a 2019 review, Ostrzenski notes that “a physiological response cannot exist without an anatomical basis,”46 however the fact that the perceived stimulation of the anterior vaginal wall elicits orgasm does not imply the existence of a particular anatomical structure.
The possible existence of an erotogenic area in the anterior vaginal wall has been referred at least since the 11th century, or even earlier.1,2
Li et al. described an increased density of microvessels and small nerves in the distal third of the anterior vaginal wall; Song et al. found higher density of terminal nerve branches at the second distal one-fifth of the anterior vaginal wall.37,33 Two other studies found no differences in the innervation of the anterior vaginal wall, but with one showing increased innervation along the urethra (which the authors did not consider evidence of the existence of the G-spot).41,42
This was a comprehensive review of the literature, including several perspectives of the question. However, the level of evidence available is low to very low, weakning the possible conclusions of the review. Since only G-spot/Gräfenberg spot was searched, it is possible that relevant anatomical studies, addressing the anterior vaginal wall were missed.


 0086-813-8127573
0086-813-8127573